Stunning Statistics and Perspective
Cardiovascular disease is the number 1 killer of women, causing 1 in 3 deaths each year, and is more deadly than all forms of cancer combined. In America, heart disease kills 7 times more women annually than breast cancer. Prior to menopause, women have a lower risk of cardiovascular disease than men of the same age. But, starting at age 40, a woman’s risk of dying from heart disease becomes greater than her risk of dying of breast cancer. Even among women who are diagnosed with breast cancer, the leading cause of death is still heart disease, not breast cancer.
In 2020, the American Heart Association (AHA) identified the menopause transition as a risk factor for cardiovascular disease (CVD). AHA along with the Menopause Society (formerly the North American Menopause Society) and the American College of Obstetricians and Gynecologists agree that for healthy, recently menopausal women, the benefits of Hormone Replacement Therapy (HRT) outweigh the risks with fewer CVD events in younger versus older women. When HRT is initiated at younger than 60 years and close to when menopause begins, HRT significantly reduces all cause mortality and confers protection against coronary heart disease and heart attacks. And as for patients with premature or surgical menopause, initiation of HRT is especially important to preserve cardiovascular health.
Accelerating Risk Factors upon Menopause
The average age of menopause is 51 and during this pivotal life stage, it is crucial that women focus on their health. This should include lifestyle modifications such as a plant-forward diet and 150 minutes of weekly exercise including strength training to optimize blood pressure, cholesterol levels, blood glucose, and body weight.
As women naturally lose estrogen with the onset of menopause, many physiological changes occur such as decreases in bone density, increased cardiovascular risk, body fat deposition issues, and increased insulin resistance. Severe e hot flashes during the menopause transition are a marker for cardiovascular disease. Also as women enter menopause, the narrowing of their blood vessels that naturally occurs with age actually accelerates, resulting in more build up of atherosclerotic plaques (fatty deposits in the inner layers of arteries). Additionally, as estradiol (the most potent and abundant estrogen) decreases, 75-80% women will have an increase of LDL cholesterol (sometimes called the “bad” cholesterol) and Triglycerides (which can raise your risk of heart disease and stroke), and a decrease in HDL (sometimes called the “good” cholesterol) without changes in diet or exercise. These factors all add up to a perfect storm for a cardiac event. It is important to note that the use of statins in women for prevention of CVD do not show a statistically significant decrease in heart attack or all-cause mortality as shown in at least 3 major recent studies.
Figure 1 – Progression of Atherosclerosis
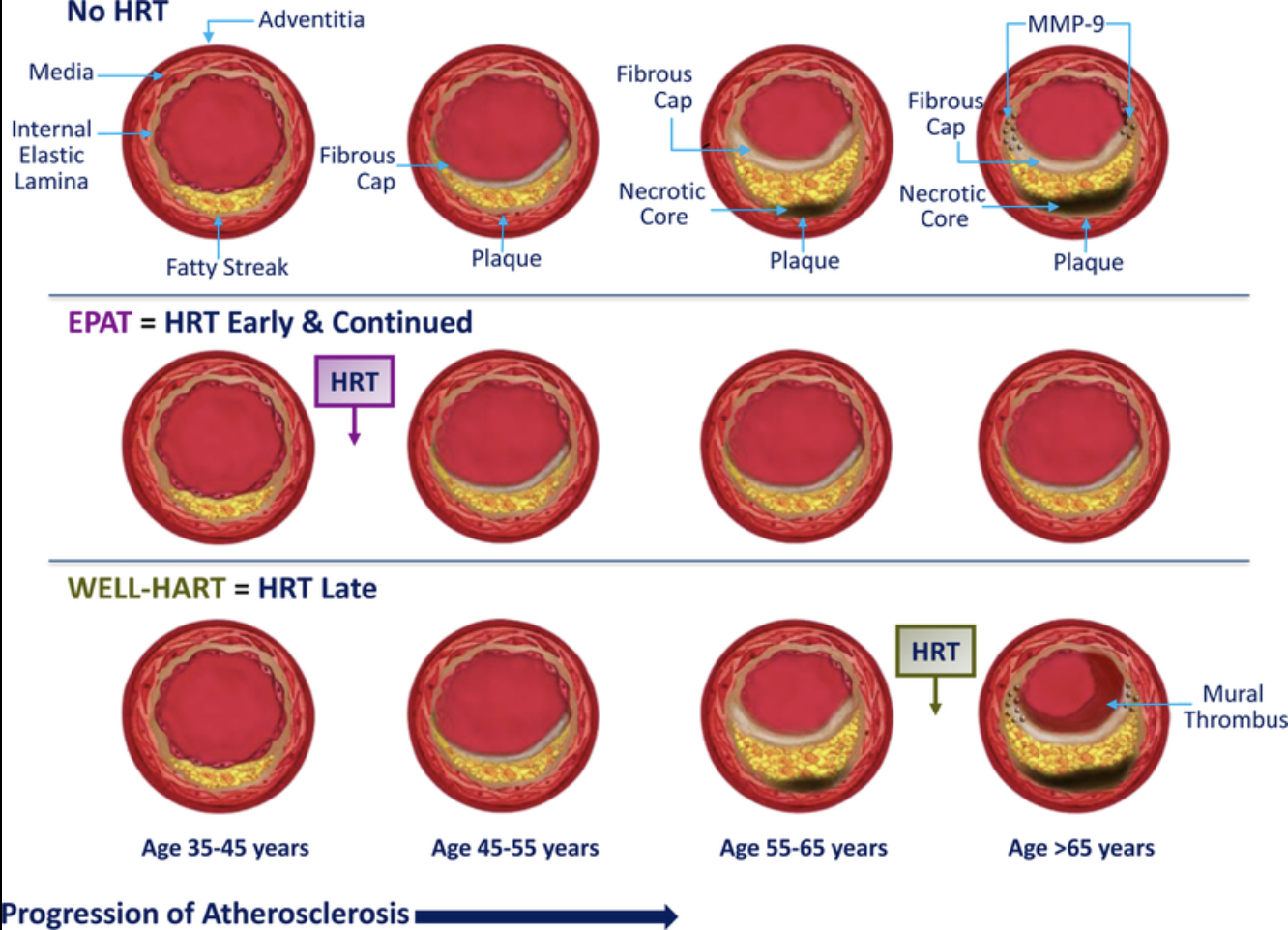
EPAT (Estrogen in the Prevention of Atherosclerosis Trial)
WELL-HART (Women’s Estrogen-Progestin Lipid-Lowering Hormone Atherosclerosis Regression Trial)
Why Initiate HRT Early After Menopause?
There is a window of opportunity, roughly defined as the first 10 years after her last menstrual period, where HRT can provide the greatest benefits. The prospective randomized Women’s Health Initiative (WHI) and the Early Versus Late Intervention Trial (ELITE) showed that starting HRT within 5 to 10 years of menopause is fundamental to the success of estrogen’s cardioprotection in post-menopausal women without adverse effects.
Epidemiologic studies have shown that estrogen replacement therapy may reduce the risk of heart disease by 30 to 50% in postmenopausal women. Estrogen is protective by modulating vascular tone, decreasing fibrosis (the thickening of heart valves), stimulating angiogenesis (the formation of new blood vessels) and vasodilation (the widening of blood vessels), enhancing mitochondrial function, and reducing oxidative stress. Specifically, the use of HRT may delay the progression of the thickness of the intima-media layer of the carotid arteries (Figure 1). That progression leads to the hardening of the arteries (atherosclerosis) and coronary calcification.
Research shows that starting estrogens later than 10 years away from menopause can be associated with a destabilization of atherosclerotic plaques. As the blood vessels narrow, estrogen could cause the clumping of platelets, which has the potential to clog an already narrowed blood vessel. This seems to be most pronounced during the first year of HRT treatment with less risk noted with each passing year. Age and length of time from the last menstrual cycle aren’t a pure contraindication for HRT, but after >10 years and >60 years old, patients and providers must carefully consider overall health and cardiovascular profile. If a patient is a healthy weight, has no cardiovascular risk factors, has good cholesterol levels, exercises, and has good blood sugar control, she could consider HRT based on individual goals such as bone health. The Menopause Society position statement supports the timing hypothesis that indicates that after more than 10 years from menopause, the benefit is less favorable with a potential greater risk of coronary heart disease, stroke, and venous thromboembolism (when a blood clot forms in a vein).
What Form of HRT is preferred?
The Menopause Society states that transdermal estradiol is not associated with any increased risk of venous thromboembolism as compared to oral. The Menopause Society also states that oral micronized progesterone is less thrombogenic (clot forming) than other progestins. Studies indicate that the bioidentical estradiol, which is the same structure as that produced by the ovaries, and micronized progesterone, which is the same structure as that produced by the corpus luteum, have the lowest risk profiles.
No studies have been conducted to determine the blood levels or dose of estradiol needed for maximum cardiovascular protection. Existing studies can also be difficult to decipher as many have utilized oral synthetic estrogens versus bioidentical estradiol, progestins versus bioidentical progesterone, and different routes of administration. Also, the FDA lumps all estrogens and progestins into 1 group. Risks are stratified based on what form of HRT is taken, the route administered, and when HRT is initiated. At this time, the data point to the preferred route for estradiol as transdermal (cream, patch, and ring) and the preferred progestin as oral micronized progesterone.
Conclusion
While the unfortunate reality is that women are still understudied, underdiagnosed, undertreated, and underrepresented in clinical trials, a few truths are emerging with regard to HRT for women:
- Data do suggest strong, consistent evidence for the beneficial effects of HRT and its long-term safety.
- Early HRT should be considered as a primary CVD prevention in women due to the reduction of all-cause mortality and lack of effectiveness of other primary prevention strategies like statins.
- The initiation of HRT before tissue damage and clinical consequences manifest appears to be key for the prevention of further tissue deterioration due to aging.
- Contraindications to initiating HRT at any time include a medical history of estrogen sensitive malignancy, stroke, pulmonary embolism, deep vein thrombosis, and unstable coronary artery disease.
Consideration for HRT must be a collaborative and individualized approach for each patient to maximize benefits and minimize risks. To learn more about the symptoms of menopause and the benefits of bioidentical hormone replacement, check out this article I wrote: Demystifying Hormone Replacement Therapy. And if you’d like to take a deeper dive into HRT, schedule a consultation with me.
If you have comments and/or questions about this blog, email us at blog@peoplesrx.com.

Deborah Fernandes is the Lead Compounding Pharmacist at Peoples Compounding Center and an HRT Specialist who has seen countless patients’ lives change for the better through compounded medications. To book an appointment for a private consultation with Deborah, click here.
References:
- Hirsch H, Iyer T. Clinical Impact of 2020 American Heart Association statement on menopause and cardiovascular disease risk. Cleveland Clinic Journal of Medicine 2022:Volume 39:13-17.
- Ryczkowska K, Adach W, Janikowski K, Banach M, Bielacka-Dabrowa A. Menopause and women’s cardiovascular health: is it really an obvious relationship? Archives of Medical Science 2023; 19 (2): 458-466.
- Hodis H, Mack W. Menopausal Hormone Replacement Therapy and Reduction of All-Cause Mortality and Cardiovascular Disease: It’s All About Time and Timing. Cancer J. 2022 May-June: 28 (3): 208-223.
- Gersh F, O’Keefe J, Lavie C. Postmenopausal hormone therapy for cardiovascular health: the evolving data. Heart. 2021 Jul;107 (14):1115-1122.
- Otto CM. Heartbeat: is postmenopausal hormone therapy a risk factor or preventative therapy for cardiovascular disease in women? Heart. 2021; 107:1103-1105.
- NAMS Position Statement: The 2022 Hormone Therapy Position Statement of the North American Menopause Society. Menopause, The Journal of the North American Menopause Society. Vol. 29, No. 7, pp 767-794.